Food preoccupation5,8
- Spending time thinking, talking about, or asking for food
- Feeling distressed if told to stop asking about food
- Food-related interruptions in daily activities
Drive to consume food5
- Bargaining to get more food
- Trying to steal food
- Foraging through trash for food
- Getting up at night to food seek
Food-related behavior problems5
- Getting upset when denied food
- Persistently asking for food after being told no
Lack of satiety5
- Consuming a significantly excessive amount of calories
- Overeating to the point of gastric rupture or necrosis
Regardless of where they are in their journey with PWS, hyperphagia impacts every aspect of life for patients and caregivers5,9
- Hyperphagia in PWS often prevents full participation in school, employment, social life, and independent living9-12
Siobhan
Daughter, friend, and dreamer taking VYKAT XR
Image
Even when weight appears to be managed and environmental controls are in place, patients may still be burdened by hyperphagia1
Connect with a representative and receive updates on VYKAT XR
Connect with usReview clinical trial data
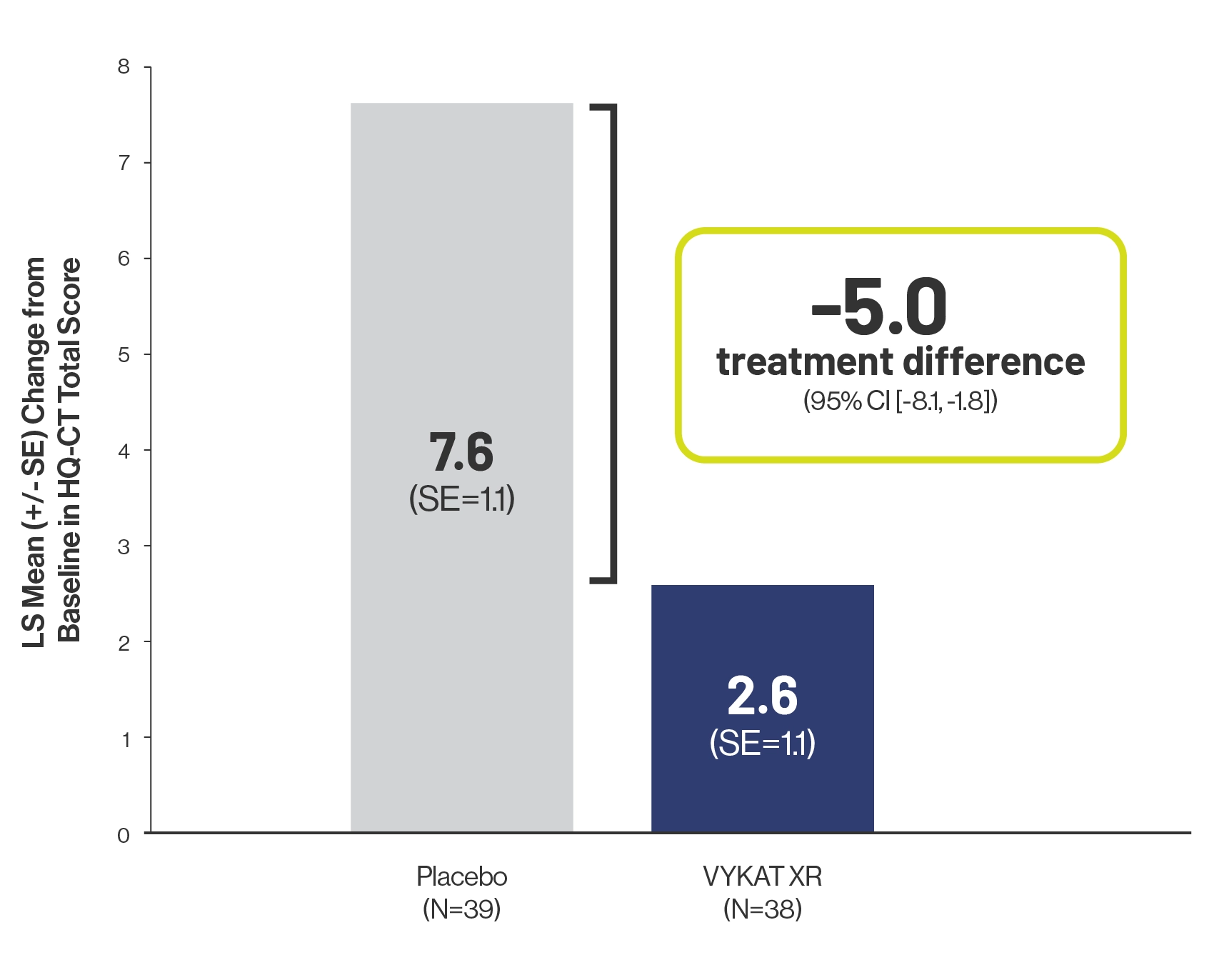
Efficacy of VYKAT XR